I was wondering about the self-selection process in testing. Pretty much only symptomatic or known exposures are getting tested, which is going to affect results. No doubt missing lots of asymptomatic or minimally symptomatic infections. It seems to me that from a public health perspective, hospital admissions would be the best measure of serious spread of disease.
2 Likes
Which is why delaying transmission as long as possible is sound public health policy. Treatment options are only going to improve with time.
You can also get closer to herd immunity by shooting uninfected people in the head. That doesn’t strike me as a wise approach either.
4 Likes
That’s changed to some extent. Our research institute is gradually reopening to lab workers, and they’re tested before returning to work and regularly (twice weekly, I think) after that.
4 Likes
Yes, it is sound public health policy, especially if we ignore the public health effects of isolation and bankruptcy and delaying vaccines and delaying “elective or deferrable” medical procedures and food insecurity.
But there are other factors that are very important, and doing everything we can do to avoid transmission is harmful to society in many other aspects.
The world is not one dimensional.
Or by isolating them until they commit suicide. That isn’t a wise approach either.
I agree.
Confirmed test counts can be a misleading measure.
And percentage of positive tests is a misleading measure if test are targeted.
That’s also confounds the results, as I think I it was in Florida, the ousted Covid official claimed that the repeated testing of negative workers made the rate of positives seem lower than it really was. Oh, well. Guess it will all work out in the end.
1 Like
Unfortunately, hospital admission can lag behind positive cases which already lag behind actual infections. They seem to only be ahead of deaths.
2 Likes
I happened to find some graphs of recent new cases and test positivity using data from the Florida Dept of Health.

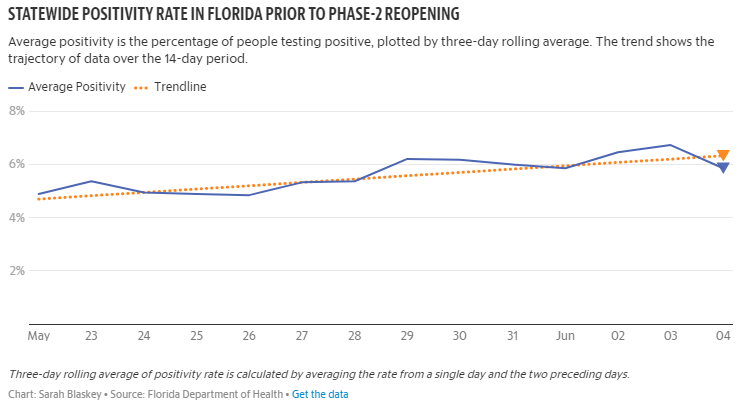
Source of graphs here.
The Centers for Disease Control and Prevention have put forth guidelines stating: Either new cases or test positivity rate needs to be in decline for an extended period before a state does phase 2 reopenings.
What epidemiological expertise do you have, Vance, such that I should weigh your opinion more strongly than that of the CDC?
Show me the data that this is happening and that it outweighs COVID-19 deaths.
And please bear in mind, as you respond, that I am not against reopening per se. I am against reopening without mask regulations and robust contact tracing.
Mask regulations are like secondary smoking regulations. Regulations that forbid smoking in restaurants, workplaces, and other enclosed spaces are a minor impingement on liberty, but the person who chooses to smoke can still do so provided that they do not endanger others while they practice their liberty. Likewise, mask regulations are a minor impingement on liberty, but the person who wants to avoid wearing a mask can drive a car instead of taking public transportation, can find a work-at-home employer instead of going to an office, etc.
Do you support secondary smoking regulations, Vance?
Thanks,
Chris
4 Likes
Right. Which it is vital to end lockdowns as soon as is compatible with keeping transmission down. Which is why public health measures that can continue to control transmission without isolation, without bankruptcy, without delaying vaccines and deferrable medical procedures, and without food insecurity are so very important. Which is why anyone arguing against a cheap, effective public health measure that accomplished all of those things would have to be extremely perverse.
I agree completely, So save a life – wear a mask.
3 Likes
Chris, I hope you do understand that simple guidelines from the CDC are:
- Part of the information weighed by those making the decisions on opening the areas;
- The health policies are only one aspect of the greater society;
- Such decisions are not and should not be made solely on an epidemiological basis; an
- Simple guidelines are just that, not rules that apply in all cases and not edicts that incorporate all the necessary information.
For example, the simple guidelines you referred to:
- did not mention whether the tests are of a randomly selected population or a targeted group of expected exposure and
- did not consider the vast difference in expected risk of the disease based on age.
I could go on, but I hope you see that such simple guidelines have some value as starting points, but your viewing them as more than they are is inappropriate.
These questions are rhetorical:
How do you weigh suicide deaths versus COVID-19 deaths? On a one on one basis? Or does a suicide affect children and relatives and spouses and parents more profoundly, because a family member may believe that there was more that he could have done to prevent a suicide? Too often suicides run in families, likely for that reason.
An alternate view is that lockdowns can fully end with herd immunity and keeping transmission rates down lowers slows the move to herd immunity.
Allowing people the freedom to make their own choices seems more consistent with human rights.
These lockdowns began with the goal of flattening the curve so as not to overrun the health care system. I supported that plan. That plan was successful. Time to move on, with people assessing their own risks and options.
Thank you for pointing out that you have exactly zero data.
I also see that you have nothing to say about the Florida data. Of course, the Florida data speak for themselves quite eloquently.
Why are you unwilling to answer, Vance?
Best,
Chris
1 Like
Key word being ‘was’ as in past tense. Some places are on pace to fill up hospitals within a month (AZ, SC,…).
You draw conclusions that are not valid.
For example, I read this study quite a while back.
“The COVID Pandemic Could Lead to 75,000 Additional Deaths from Alcohol and Drug Misuse and Suicide”
My unwillingness to answer every question asked is a matter of priorities, not an indication of anything else.
Should that affect other areas?
That’s a projection for what could happen over the next ten years. The projection is based on some evidence of how unemployment and suicide are linked but it’s not data.
What do you mean?
Which specific regulation?
There should have been a question mark on the end. I added the question mark with an edit.
It means: should a localized area’s higher infection level affect the freedoms in different areas?
For example, should the “disease load” in Albany Georgia have resulted in isolation and loss of freedoms in Dillard Georgia, around 300 miles away?
Arizona is a big state, too.
My daughter lives in a city with a few hundred thousand people in Canada. When I talked to her last week, there were two cases in the city. But the city is shut down. That seems an overreaction. Well, not completely shutdown, as the government employees are still working.
If you desire to dismiss projections because they aren’t “data,” that does limit your objections to projections of what might happen without masks and sheltering-in-place, doesn’t it?