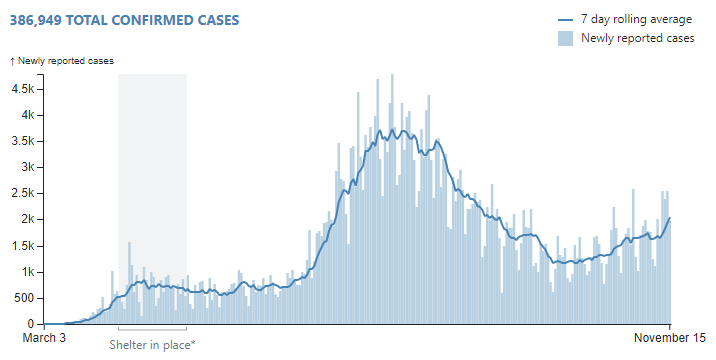
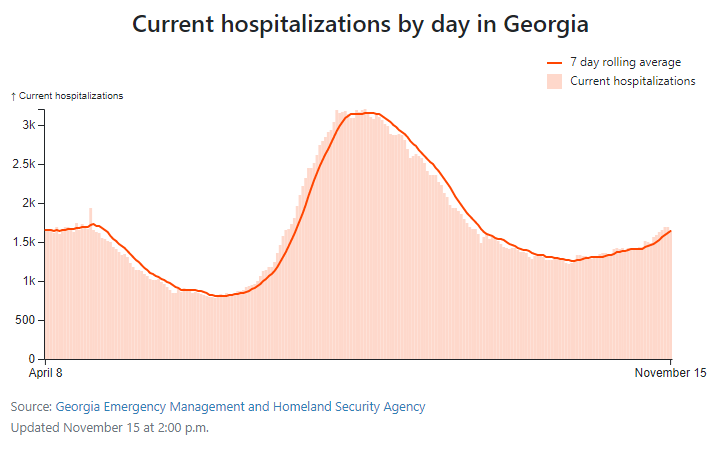
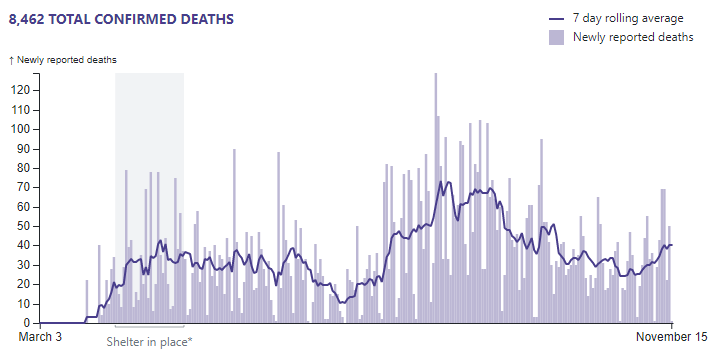
We have had some discussions on the forum as to whether the population of Georgia (USA) might be approaching herd immunity. Unfortunately, it seems that the hope for immunity has not materialized; the COVID-19 crisis has been deepening in Georgia over the past month (as it has almost everywhere in the United States). Cases started increasing at the beginning of October; 10 days later, hospitalizations started increasing; and two weeks after that, deaths started increasing. Since hospitalizations lag cases and deaths lag hospitalizations, it seems that things will get worse before they get better.
We have friends on this forum who are citizens of the Peach State (I hope you and yours are staying safe, @03Cobra!). My daughter lives in Georgia, so I am always hoping for the best there.
Hospitalizations are a better measure than confirmed cases, since confirmed cases are a function of testing. Hospitalizations measure serious sickness.
There are 2 sources of the discrepancy. Both are important, but I do not know which would be more important:
The CDC data reflect only a quarter to a half of the population of Georgia that are served by hospitals that participate in COVID-NET. The data I cite are for the entire population of Georgia. The CDC sample is definitely not random because it skews toward hospitals with the resources to participate in the sophisticated COVID-NET data gathering operation.
The data @03Cobra cites are significantly lagged. The amount of lag is not specified, but the CDC data are clearly far behind the data I cited.
Your assertion is a truism to the extent that if there are zero tests, then there will be zero confirmed cases.
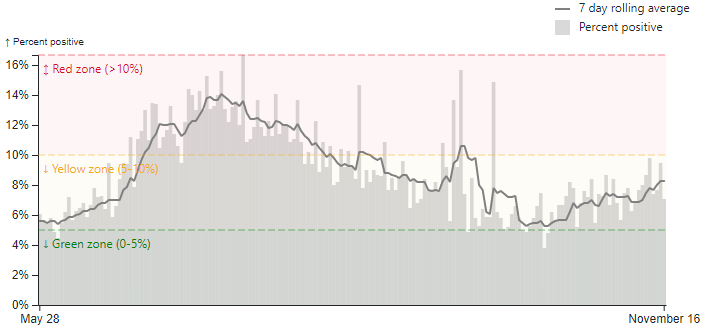
Where adequate testing is available (as in Georgia), increased testing should result in a lower positivity rate ceteris paribus. So let’s examine the trend in test positivity (same data source as the OP):
Ouch! This is very unfortunate: Test positivity has risen from 5% to 8% over the past few weeks. This is a very strong signal that the COVID-19 crisis is deepening in Georgia.
It is obviously true, but it is also interesting — so it is not a truism.
The fact that people point to confirmed cases as evidence of a crisis without noting that the number of confirmed cases is a function of testing is often a tool of those who desire to mislead.
Test positivity is also a function of the subset of society that is tested, as testing is not random.
Well, if a certain crew hadn’t hyped that particular truism, decrying a nationwide mask mandate (yes, Vance, allowance can be made for rare exceptions), the country wouldn’t be in as severe a crisis as it is now. Of course more testing will find more positives. Certain people were saying “Test less, and the virus will disappear!” Talk about misleading and misleadership (or misternotleadership).
It is always easy to predict what would have happened if some other path had been taken, but it is not always accurate nor is it always encompassing of the other effects.
I guess the epidemiology faculty at Johns Hopkins University must be perniciously trying to mislead us; they disagree quite pointedly with your assertion, Vance.
there are two ways to lower the percent positive: Reduce the amount of coronavirus transmission or increase the number of people who get tested.
The percent positive is a critical measure because it gives us an indication how widespread infection is in the area where the testing is occurring
a high percentage of positive tests suggests high coronavirus infection rates (due to high transmission in the community), a high percent positive can indicate it may be a good time to add restrictions to slow the spread of disease.
Vance, you can go on citing your Ph.D. epidemiologist, Donald John Trump, all you want. But I prefer to listen to the epidemiologists at Johns Hopkins.
Dale, I don’t think you have considered the differences between the populations of Europe and the US and how those populations differ in demographics and health.