While this study was not done with adequate controls, by researchers with known track records or appropriate credentials, or with adequate numbers to see a statistically significant response, it does peek one’s interest and makes looking further desirable. The fact that when looked at with greater numbers and with closer examination though with slightly different criteria, no improvement was seen makes it seem a waste of time and money, however.
2 Likes
As someone’s aging loved one I appreciate both of your concern. Fortunately I do not believe there is anything which can confer immunity to COVID on me, except perhaps a vaccine but we’ll wait for testing before letting our guard down even then. People are too eager to trust their camel to God. Why not just tie it securely and take one more task off God’s to do list?
1 Like
A glass of milk is even safer for those who are lactose tolerant. Why don’t we prescribe milk for COVID-19 patients?
That’s not what studies have found:
2 Likes
I was thinking of my parents. Mom is gone but Dad is 97. As they aged they gradually became careless about medicine, refrigerating perishables, and other stuff.
- Watanabe’s meta-analysis was of Boulware’s study.
- The first Barcelona study is the one that Risch refers to in the opening post, where it prevented Covid-19 in over half the nursing home patients - the high risk group.
- The second study is of mostly younger, low risk patients, who usually recover without treatment. So difficult to show advantage for HCQ. Unless they want to stratify the results and show us how it fared for older, high risk patients.
The question is always one of cost/benefit. Thousands of people are dying everyday. Do we risk using a 65 year old drug that we know is safe when used for other diseases in order to try to save those thousands, or do we let them die while we try to find out it if HCQ is safe to use first. So far, hospital trials show it to be safe for Covid-19. Why think it will be different in outpatients?
But you just argued that it should not be used with very sick people, it should be used with not so sick people. The vast majority of whom will recover with no drug. This whole “it could save someone’s life” is total speculation. That would only apply to a very small minority. The side effects that might kill them also apply to a small minority. It’s not honest to pose the situation as offering a life-saving treatment. In the scenarios where people’s lives needed saving, Hydroxychloroquine was not effective and probably was detrimental, according to multiple studies. Your cost/benefit analysis is based on wishful thinking, not real proven benefit, or known costs.
3 Likes
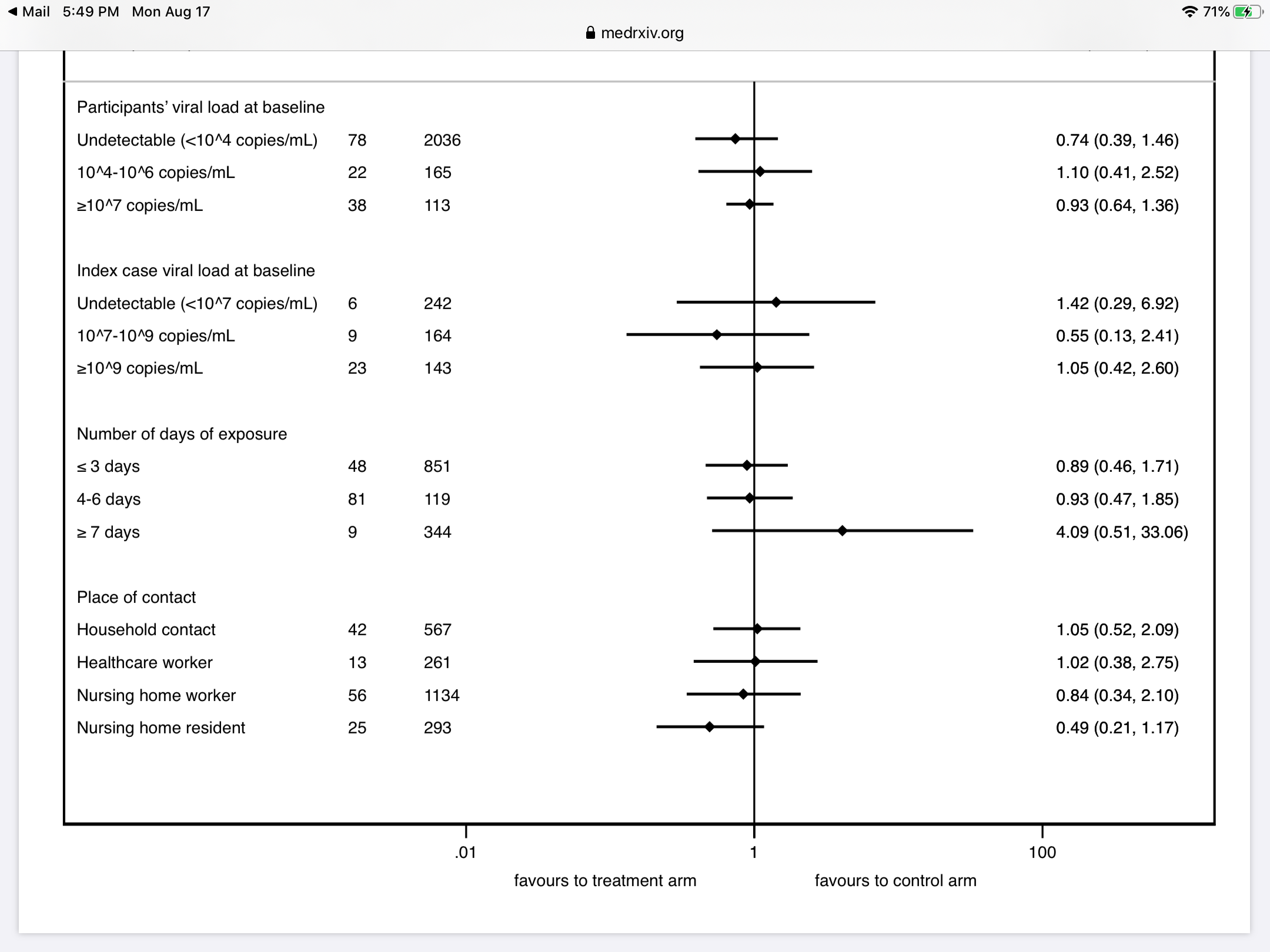
I’m not seeing that information in the paper:
They used PCR tests, not symptoms. HCQ did not prevent infection as determined by the presence of virus.
2 Likes
HCQ is not that effective with very sick Covid patients, because the disease has changed from merely viral to pneumonia, very often with a cytokine storm. HCQ is most effective in stopping viral replication, which means it should be used early in the disease, before it progresses to pneumonia. High risk outpatients - the elderly or those with serious comorbidities - are the ones who especially need to be treated early.
In that group, the 95% confidence interval overlaps with no effect. There was no statistically significant effect from HCQ treatment.
3 Likes
Because the sample group was too small.
Yes I agree that the data shows that early intervention with hcq may be beneficial in preventing the severe symptoms and it may also prevent the 10- 15 % symptomatic patients that go on to have long term complications ( just speculation no data for that yet). You are right that the focus should be on the high risk to administer early as possible along with zinc. Doctors all over the place are looking at this data and familiar with the drug and can’t believe how it became politicized. We should learn from what happened with the steroids and the placing of restrictions on this hcq drug has been a blemish on our medical systems response to this pandemic.
It may be anecedotally interesting that Covid 19 also binds the cd 147 molecule (targets T cells and red blood cells) which also is the target protein on cells for the malaria parasite that the hcq is used to treat… This virus has a bunch of tricks in it’s design.
We have to consider that the antiviral remdisovir also would be a good candidate for early intervention but due to low availability and high cost this is not feasible. There are a number of other good early interventions that we should be aggressive with this high risk population but also as mentioned anyone that gets the virus should be starting treating early to prevent severe symptoms and possibly long term complications.
How do you explain that in countries where there has been no “politics” around the drug, doctors are not rushing to prescribe it. If it was just a matter of political roadblocks preventing a good option in the US, don’t you think some other countries would be pushing it harder?
I believe countries like India and others are using the drug however, the WHO saw data of late use adverse events and decided to withdraw support of the drug. It’s clearly not indicated for late use but the data may show benefit early on. I don’t think that hcq is a what was it a game changer at all and needs better studies but it’s not the dangerous drug made out to be either. Studies were showing it more effective with zinc and none of these trials mentioned were done with zinc. It not surprising that as we learn more about Covid we determine what works when and on who it works. There’s probably a time and place for hcq for now at this stage until we have better interventions. The iv steroids are not indicated for early use but now we are seeing studies showing that inhaled steroids may be of benefit to prevent severe symptoms. The thrombosis that’s occurring is not classic pathway and not responding well to traditional medications and requires that we understand it and prevent it. There’s lots of stuff coming out and the virus attacks in many ways and so we need to be flexible to understand that and allow the frontline medical providers to respond as needed .
It’s because the effect, if there is any, is too small
3 Likes
There is no data demonstrating HCQ has any significant effect whatsoever. However, there are other drugs that have shown promise and those are the ones that we should be focusing on. The only reason HCQ is being trumpeted on online forums is politics.
My irony meter just exploded. Perhaps you aren’t familiar with American politics? Perhaps you haven’t heard of a certain US President who touted the drug with no evidence to back it, and now his followers are trying to support their dear leader by falsely claiming HCQ is effective?
3 Likes
Sorry but I am not political and don’t care about Dr trump. The steroid fiasco should be a lesson to us. It cost tens of thousands of lives and was a terrible mistake. When the data came out from the uk that steroids were highly effective reducing mortality by at least 30% in icu patients many doctors in US were dumbfounded by this as the cdc and who were advising against steroid use. It cost thousands of lives in ny alone. Doctors couldn’t believe the ny data and then there were some doctors that were incredulous saying that they had been using it all along elsewhere and couldn’t believe people were not using it.
As mentioned virus attacks in many ways but there is a basis that the hcq with zinc may be effective early on and is not dangerous. The risk benefit should be in the doctors hands to assess this not by some governor or politician to determine.doctors are familiar with this drug and understand its contraindications.We don’t understand this virus well enough and there are no good trials one way or the other for its benefit. We also don’t know whether this drug may prevent long term complications that amounts to about 15% of symptomatic. We need to let our doctors be doctors in this emergency situation understanding the risk benefit to their patients particularly the high risk patients treated early.
As I have said it’s no game changer and shouldn’t even be such a big deal as there are other early interventions emerging that some doctors are using that are seeing good results. Just the same since this virus is not one size fits all hcq is something a doctor should be able to prescribe as they think necessary.
The data is out for HCQ, and there is no evidence of efficacy. So why is it still being pushed?
The data shows that it isn’t effective.