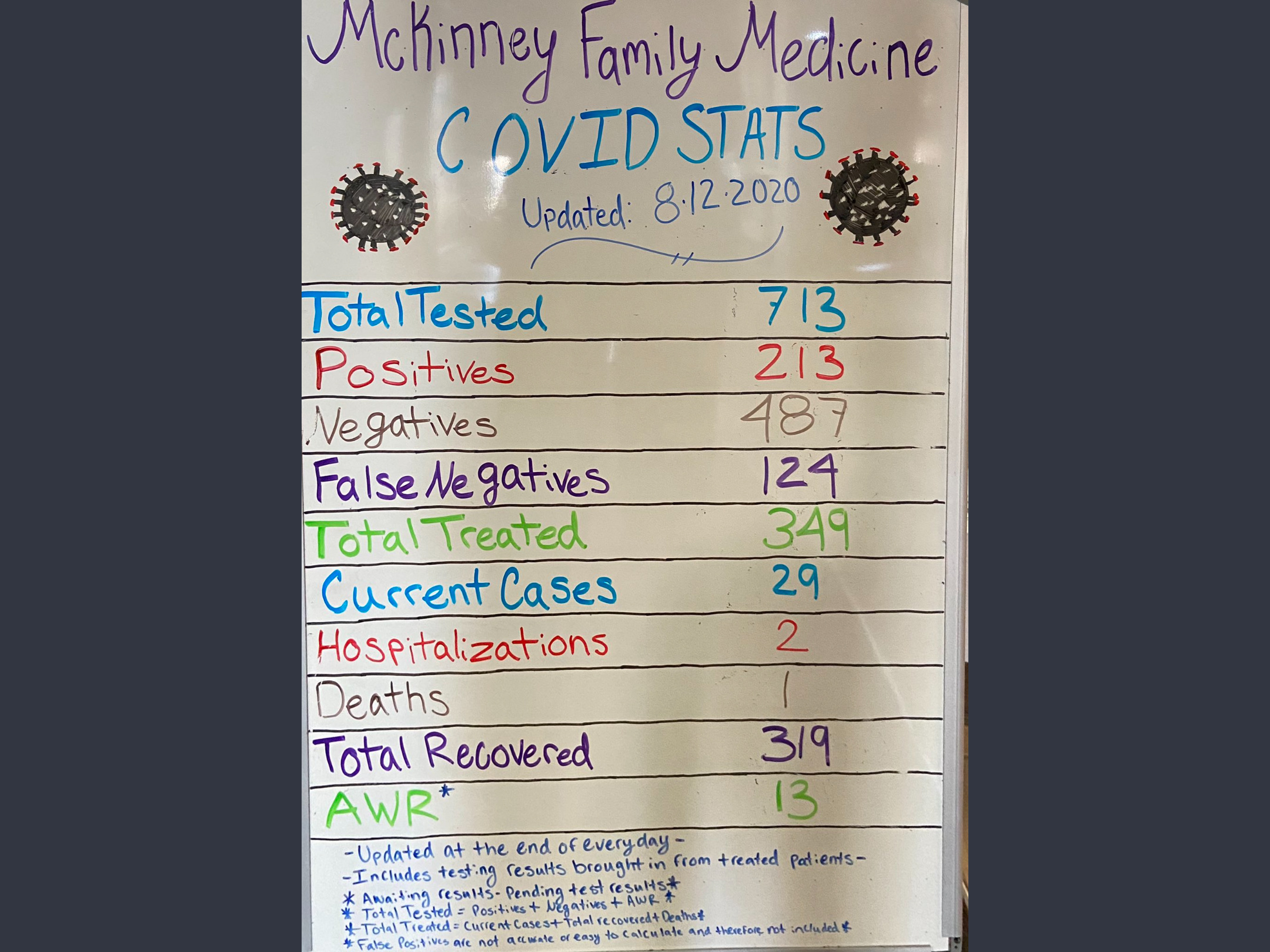
I’ve been following Dr. Brian Charles Procter, who updates his stat board daily. He states that 196 of these patients are in the high risk group (over 60 or having at least one comorbidity):
A short video from one of the ophthamologists:
There are a lot of things that can bias results which is why you can’t learn much of anything from such data. Like what kinds of people go to the McKinney Family Medicine practice in the first place? While supposedly 196 patients are over 60 or have one comorbidity, we need a LOT more information. You should be asking which comorbidities, what is the increased risk with that comorbidity? Like if someone is 20 years old there’s about one death in every 3,000 cases. And if they have one comorbidity, let’s say that increases their risk of 10%. Then there would be one death in every 2,700 cases. One cannot rely on such stat boards to demonstrate the efficacy of anything.
He’s an ophthalmologist to begin, but doctors shouldn’t be able to just give whatever medication they want to patients if it does not have sufficient evidence of efficacy and leads to increased adverse effects (not necessarily “serious” but still more than a control group).
4 Likes
Here’s the latest cure from the White House:
https://www.axios.com/trump-covid-oleandrin-9896f570-6cd8-4919-af3a-65ebad113d41.html
Sad and pathetic. But note @EricMH it isn’t scientists pushing the whack but politicians and grifters.
My parents always warned us strongly as kids never to put anything from poisonous oleanders near our mouths. That’s about all I know about that, but it scares me that someone might push that over the counter.
No, in the cases I mentioned it is precisely the scientists pushing the whack. Should laypeople listen to the experts when they are pushing the whack?
they should always follow their own rules. If they don’t, they should face consequences. Physicians should; so should scientists. I am having trouble finding your post–which one was it? Sorry.
Thanks.
In the past century, scientists have push eugenics and racism. I claim the lay people of their time were well within their rights to reject the claims of these experts. Would you agree?
Well, we talked about GK Chesterton struggling with the same period specific baggage (I imagine we have the same sort of baggage, or will have when inspected by those who come after us). We should always try to self introspect, and certainly working beyond our scope of practice (eg in eugenics, when that’s not their training) would be a great thing to avoid. Am I responding to your good question? Thanks.
Would GKC be right to reject the racism promoted by the scientific experts of his day, as he did in the person of Father Brown in God of the Gongs:
https://www.gutenberg.org/files/223/223-h/223-h.htm
“Malvoli,” said the priest, “has nothing to do with it. I dare say he has some Italians with him, but our amiable friends are not Italians. They are octoroons and African half-bloods of various shades, but I fear we English think all foreigners are much the same so long as they are dark and dirty. Also,” he added, with a smile, “I fear the English decline to draw any fine distinction between the moral character produced by my religion and that which blooms out of Voodoo.”
GKC does not attribute the cannibalism to the scientific racism of his day, but to the religion adopted by the cannibals, in stark contrast to the experts.
Was GKC right to do this?
1 Like
HCQ is an over the counter medication in many countries, especially where malaria is present. Tylenol is much more dangerous than HCQ. These are doctors trying to save lives during a pandemic. Instead of telling their patients to go home and wait until they are sick enough to be admitted to the hospital, they actually try to treat them before the virus is out of control. That is what standard medical practice calls for for other deadly viruses. And they are having success with HCQ, AZ or Doxycycline, and Zn. None of you want to believe them. Instead, you want to wait until RCTs are done. By no RCTs are being done on high risk outpatients. And those are the ones who needed to be treated early, before the virus grows out of control. So treat, or wait until the patient is sick enough to go to the hospital? Doctors who care treat. And have tremendous success.
But doctors who don’t care and don t treat or care and don’t treat also have tremendous success, so there is the problem.
2 Likes
Is this because while hundreds of thousands catch the disease it only kills in the thousands?
Yeppers. So an individual physician may well treat hundreds of patients before one of them by chance happens to die.
2 Likes
Scientifically designed clinical trials have not seen success, be it treatment or prevention.
Good comment with good insight, but does this help? Tylenol is very safe in levels below the recommended maximum. I’m not tackling the chloroquine issue (I took it as a child, but I am not advocating its use). Just wanted to point out that Tylenol is very toxic over the recommended dose, but not at regular doses. Does that help? thanks.
1 Like
This topic was automatically closed 6 days after the last reply. New replies are no longer allowed.