Am I the only one out there who has observed many from the NIH seemingly communicating the party-line rather than sticking to what the science is saying?
Example from www.protectpublicstrust .org:
Bret Baier: “Can you definitively say to somebody that the vaccine provides
better protection than the antibodies that you get from actually having had
Covid-19?”
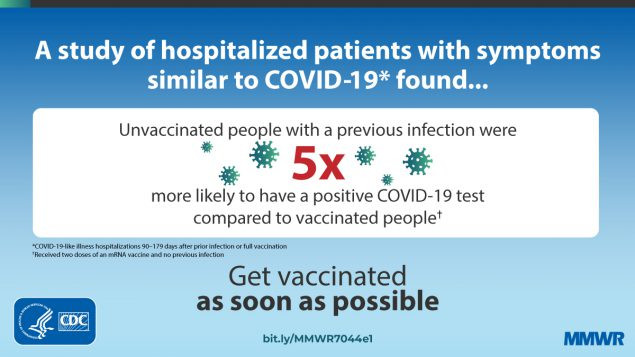
Francis Collins: “Yes, Bret, I can say that. There was a study published by CDC
just ten days ago in Kentucky. And they looked specifically at people who had
had natural infection and people who’d been vaccinated and then ended up getting
infected again. So what was the protection level? It was more than two-fold better
from the people who had the vaccine in terms of protection than people who’d
had the natural infection. That’s very clear in that Kentucky study.”
Collins’s reply evoked strong responses from the scientific community for misstating the study’s conclusion. Dr. Martin Kuldorff, another highly respected epidemiologist at Harvard Medical School, critiqued Dr. Collins on this point.
On natural immunity, NIHDirector Francis Collins is misleading the public.
Kentucky study shows less reinfections after COVID disease plus vaccine than
COVID only (both very low). He falsely claims less reinfections after vaccine
than after COVID disease.
Furthermore, CDC’s highlighting the results of a carefully selected two-month period from a single state (out of a 50 State study) led Dr. Marty Makary, a Johns Hopkins University Surgical Professor, to claim the CDC was “fishing” in order to find support for a policy position promoted by political leadership at the agency and at the White House. While policy positions are wholly within the discretion granted to political leadership, they must not conflict with the applicable
scientific integrity policies. It is not clear they cleared this bar. Dr. Makary also noted the exceedingly low infection rate of the subjects, among both vaccinated and unvaccinated, in the Kentucky study.